



Itinerary: In-brief
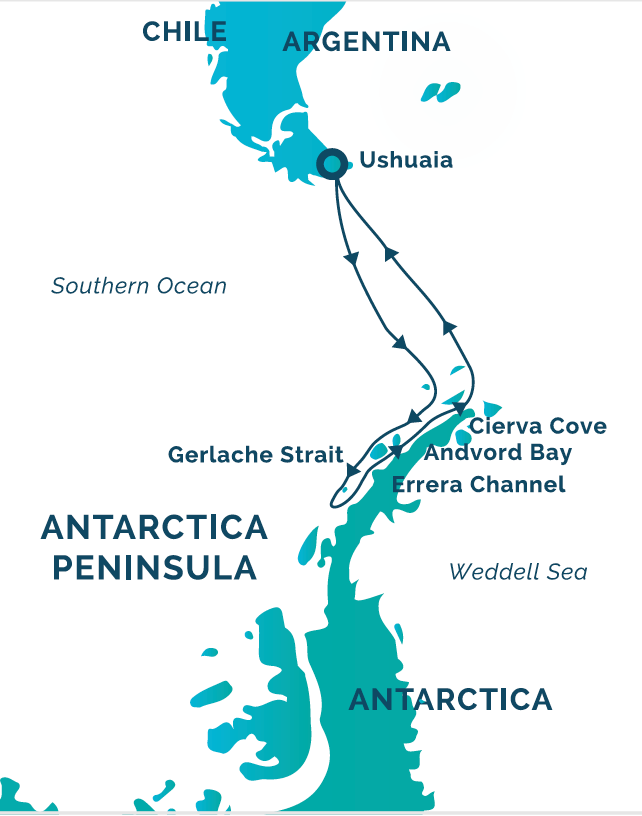
Day 1 Arrive in Ushuaia, Argentina, Arakur Resort & Spa
Day 2 Arakur Conference Room: Form & Force Closure, Principles of ISM and the pelvis (full day) meet for dinner in the Arakur resort
Day 3 Arakur Conference Room: An introduction to the Thorax and its role in pelvic control (1/2 day followed by a walk on the resort conservation area after lunch)
Day 4 Embark on the boat, watch the 1st lecture on Pregnancy & the Abdominal Wall on own time. Wildlife presentations Sea Spirit
Day 5 Cross the Drake Passage! Practical Discussion from 1st lecture, watch the 2nd lecture Anatomy of the Abdominal Wall on own time. Birdwatching, ship presentations
Day 6 Continue to cross the Drake Passage. Practical Discussion from 2nd lecture, watch 3rd lecture Function of the Abdominal Wall on own time. Bird watching, ship presentations
Day 7 Antarctica: Walking amongst Penguins, Zodiac rides, icebergs, whales, seals. Practical Discussion of 3rd lecture, watch the 4th lecture 2016 DRA trial
Days 8-11 Antartica experience continues with each day review having Practical Discussions of the previous night’s self watched lecture (5th is DRA in men & kids and surgery, 6th is Part 1 of Assessment, 7th is Part 2 of Assessment, 8th is Training of the Abdominal Wall. Each day there will be walks and Zodiac rides with lots of social time.
Days 12 & 13 Return across the Drake Passage and our Practical Discussion time will be weather dependent
Day 14 Arrive Ushuaia and Fly home
Days 1 & 2 (1/2 day)
1.5 days on land and then 12 days on the Sea Spirit to cover the following in a combination of lecture video (own time) and practical discussion format
Thoracic Pelvic Girdle Pain & Dysfunction – The Form & Force Closure Mechanisms for Pelvic Control – 30 years of Research to Clinical Practice (1993-2023)
The form and force closure mechanisms for how loads are transferred through the pelvic girdle come from the pivotal research of Dr. Andry Vleeming, Dr. R Stoeckart, Professor Chris Snijders in the early 1990’s. These mechanisms provided evidence for the clinical tests of both passive and active control of the SIJ that were evolving in clinical practice concurrently (Diane Lee, Dr. Barb Hungerford).
Subsequently in the mid-90s and ongoing, the understanding of how force closure of the pelvis can be impacted by motor control strategies, pain, trauma and certain emotional states, broadened our clinical assessment and a true biopsychosocial model for managing pelvic girdle pain and dysfunction has evolved.
What remains to investigate, and is being considered today in clinical practice, is the impact remote impairments can have on these mechanisms of pelvic control. In other words, can clinicians reliably determine that the pelvic girdle is a victim of impairments elsewhere?
The pelvic girdle is part of the whole body/whole person and this workshop will focus primarily on the clinical application of the evidence to date (assessments of form and force closure mechanisms, motor control strategies and myofascial impairments (DRA)) after briefly describing a regional interdependent approach (the Integrated Systems Model (ISM)) that helps determine when to treat the pelvis and when to look elsewhere to improve strategies for effective load transfer.
Theory & Evidence
- The Beginning: 1990 – 1993 the research that led to the form and force closure mechanism models for pelvic control (Vleeming, Snjiders, Stoekart)
- The Middle: 1995 – 2012 the research that improved our understanding of the force closure mechanism (motor control transversus abdominis, pelvic floor, sacral fibres of multifidus (Hodges, Sapsford, Hides & more) and led to the Integrated Model of Function (Lee & Vleeming) and ultimately recognition that pelvic girdle pain/dysfunction is not always caused by the pelvis (The Integrated Systems Model) (Lee 2011)
- The Present: 2012 – 2023 How understanding the phenotypes of pain, and the impact trauma and the emotional state in relationship to threat/safety has on pain and motor control, facilitates choice of approach to patient care (biomechanical & motor control (movement based) vs cognitive-behaviour approaches)
Morning tea
Knowledge Translation – From the Evidence to Clinical Practice (Part 1)
- The Integrated Systems Model – A Regional Interdependent Model to understand when the pelvis is a victim of impairments elsewhere
- When the pelvis is the driver/problem (will practice these tests):
- Further assessment of the Form Closure Mechanism – Active and Passive Mobility, Passive Control tests for the sacroiliac joint and pubic symphysis
- Further assessment of the Force Closure Mechanism – Active Control tests for the SIJ & pubic symphysis
Lunch
Knowledge Translation – From the Evidence to Clinical Practice (Part 2) 1
- Motor control analysis of the deep muscle system of the pelvic girdle (demonstration)
- Low fibres of transversus abdominis – clinical tests and ultrasound imaging
- ii).The pelvic floor – iliococcygeus & coccygeus – when to refer to a pelvic health physiotherapist
- ii).The sacral fibres of multifidus – clinical tests
- Diastasis Rectus Abdominis (DRA): Impact of a low DRA on the force closure mechanism of the pelvis – demonstrate clinical tests for myofascial integrity of the lowest part of the linea alba
Afternoon tea
Knowledge Translation – From the Evidence to Clinical Practice – Part 2
- Clinical reasoning of clustered test findings (form & force closure and motor control tests) to guide individualized patient management
- Manual treatment techniques to release the restricted SIJ – demo or video
- Progressive stages of exercise training to restore motor control and the force closure mechanism – discussion
Thoracic Impairments and Pelvic Control: When to Treat What? Translation of the Motor Control Evidence into Clinical Practice
Several studies have shown that motor control changes in response to pain in the trunk are highly variable and the consistent finding is a redistribution of muscle activity with deep muscles becoming inhibited and superficial muscles augmented (Hodges & Smeets 2015). The superficial muscles connect the thorax to the lumbar spine and pelvis and can potentially limit mobility, and reduce control, of the individual thoracic rings, lumbar spine and pelvis. While poor pelvic control is often addressed with motor control training, the individual thoracic rings are often not considered as part of this training. Additionally, there are no studies that have considered the role of sub-optimal alignment, biomechanics and control of the thorax on pelvic control. Therefore, in persistent pain conditions such as low back or pelvic girdle pain, understanding the role of the thorax requires an innovative, individual clinical reasoning approach that is evidence-informed.
This lecture/practical will introduce tests to
- determine when the thorax is playing a critical role for an individual with impaired function of the pelvic girdle (loss of mobility and/or control) with or without pain.
- differentiate which manual therapy techniques are indicated for the impaired thoracic rings
- predict the impact of treating the thorax on pelvic mobility & control
This is a combination of lecture, case videos and live demonstration/practice when possible of manual assessment skills for determining
- mobility/control of the 3rd to the 10th thoracic rings
- the relationship between sub-optimal alignment and biomechanics of the pelvis on the thorax as well as the thorax on the pelvis
- whether the mobility restriction of the thorax is secondary to an impairment in the
- articular
- neural, or
- myofascial systems
- which manual therapy technique to use to restore optimal mobility of the relevant thoracic ring
Lectures/Discussion on the Sea Spirit
The Abdominal Wall – Implications for Assessment and Treatment of Thoraco-Lumbar-Pelvic Pain & Disability
Impairments of abdominal wall anatomy and function have been implicated in multiple conditions associated with pregnancy and delivery including low back and pelvic girdle pain, urinary incontinence, pelvic organ prolapse and diastasis rectus abdominis (DRA). DRA is a common occurrence in pregnancy and postpartum, it does not completely recover in some, and the current evidence has not clarified the risk factors for this condition, nor provided direction for treatment. The lectures (own time) and practical discussion onboard will:
- present the current research evidence on the prevalence, risk factors known/not known and the course of recovery of DRA,
- discuss the anatomical variations of the upper, middle and lower abdominal wall, particularly the aponeurotic extensions of the lateral muscles in all three regions and how they form the linea alba,
- discuss the role of the abdominal wall in function of the thorax, lumbar spine and pelvic girdle in all individuals,
- define and suggest a classification model for subgrouping women with DRA both for research and clinical practice,
- illustrate the clinical tests for determining if the individual’s strategy for transferring loads through the thorax, lumbar spine and pelvic girdle is optimal (i.e. is their motor control strategies and force closure mechanisms optimal for function),
- clinically reason the load transfer test findings to determine which level/region of the abdomen (upper, middle lower) requires further assessment,
- demonstrate the clinical and ultrasound evaluation of the lateral and midline abdominal muscles as well as their connective tissue connections to determine if the myofascial system can transfer loads. These tests consider the following parameters for function:
- anatomical integrity
- motor control
- strength and endurance capacity,
- discuss current clinical thoughts on who should be referred for surgical repair and who should respond to treatment/training
- present the 3 stages of motor learning training (cognitive, associative, and automatic) for the abdominal wall and how to progress this training for strength, endurance and function
Reviews
There are no reviews yet.