Introduction
In clinical practice, it is common to see complex patients with a combination of impairments in multiple systems including the musculoskeletal, urogynecological and respiratory. A thorough evaluation often reveals many past injuries, thoughts/beliefs, emotional states and movement habits that have collectively led to changes in strategies for posture, movement, continence and respiration.
Every individual with lumbopelvic pain has different sensorial, cognitive and emotional dimensions unique to their experience and this individual nature of the complex patient is supported in that there is limited data of a direct relationship between the various system impairments, location of pain, or motor control strategies (Hodges, McGill & Hides 2013, Moseley 2013). Randomized controlled trials have not provided answers for the management of the individual patient.
There was a promise that randomized controlled trials could provide answers on questions such as ‘which intervention is most effective for which patient’, but after the publication of more than 1000 randomized controlled trials on low back pain there is still a lack of evidence regarding the most effective strategies for matching individual patients to particular interventions. The Cochrane Back Review Group acknowledged the limited role of randomized controlled trials in providing useful information on aspects of low back pain management… Trials of non-specific low back pain that fail to consider the heterogeneity of back pain presentation should be discouraged (Van Dillen & van Tulder 2013).
In her opening keynote address at IFOMT Professor Gwen Jull said that the ‘future [of physiotherapy] continues with an informed clinically reasoned assessment approach to direct management of the individual patient’ (Jull 2012).
It is felt that
an advantage of the individual clinical reasoning approach is that it can allow the therapist to be more sensitive to unique characteristics of patient in front of them, rather than being biased by expected features of a subgroup. Although many patients are neatly classifiable into a subgroup in one approach or another, others do not so easily fit within the expectations of an approach (Hodges, Van Dillen, McGill, Brumagne, Hides & Moseley 2013).
Related Lecture
Acute back pain patients often have similar histories but present at a different stage of their condition. Ultimately, best conservative care should consider, and address, the role each system and body region is having on the collective cortical body-matrix.
More InfoFREE
The Integrated Systems Model
The Integrated Systems Model approach (ISM) (Lee L-J & Lee D 2011, Lee 2015) is an evidence-informed clinical reasoning approach that considers all three dimensions of the patient’s experience to facilitate decisions for individual management. This approach provides clinicians with a framework to help organize knowledge (theoretical, scientific and experiential) and develop clinical reasoning skills for treatment of the whole person/body.
The Clinical Puzzle
The Clinical Puzzle (Lee & Lee 2008) (Fig. 1) is a graphic conceptualization of the Integrated Systems Model and represents the person and their problem(s) (center of the puzzle), and the body systems that support optimal strategies for function and performance (articular, neural, myofascial, visceral (individual pieces) and physiological (center)). The Clinical Puzzle is used to reflect on key findings from the assessment (organize the information) to clinically reason and plan best management.

The ISM approach is applicable to disability with or without pain (peripheral or centrally mediated) of any duration (acute or chronic) and is centered on the patient’s values and goals, a key component of evidence-based, or informed, practice (Sackett et al 2000). The assessment is meaningful to the patient’s story and is not protocol-driven or based on clinical guidelines or prediction rules for regional pain. Determining what has meaning for the individual patient (i.e. what they think, feel and believe) and how they are ‘experiencing’ their body is a critical first step in the assessment.
Melzak describes the gestalt of one’s experience as follows:
The body is felt as a unity, with different qualities at different times….[Together all outputs] produce a continuous message that represents the whole body… felt as a whole body possessing a sense of self… as a flow of awareness (Melzak 2001, 2005).
The Body-Self Neuromatrix

The body-self neuromatrix (Fig. 2) (Melzak 2001) is useful for understanding how inputs to the matrix (the whole body nervous system) from:
- Cognitions (memories of past experiences, what we focus our attention on, what has meaning, beliefs),
- Sensations (cutaneous, nociceptive, visceral, musculoskeletal etc.), and
- Emotions (fear, hyper vigilance, anger, sadness, grief)
lead to outputs potentially producing:
- Pain
- Involuntary and voluntary action patterns (i.e. redistribution of activity within and between muscles (Hodges 2011), and/or
- Activation of the stress-regulatory system (cortisol, nor-epinephrine and endorphin levels, dampening of the immune system).
The outputs are essentially related to the sympathetic nervous system’s flight, fight, or freeze response to threat or perceived risk of threat. No two individuals will have the same experience or behavior in response to threat (real or imagined) because how they manifest their pain or illness is shaped in part by who they are, what they think, and how they feel (Jones & Rivett 2004). Understanding the individual with chronic lumbopelvic pain begins by hearing their story and understanding all three dimensions of their experience.
The Patient's Story
Key features from the patient’s story are noted in the center of the Clinical Puzzle including:
- The patient’s meaningful complaint – the primary symptom (thoughts, emotions, sensations).
- The patient’s meaningful task/goals – the aggravating posture or movement (“I have low back pain when I run”), tasks which are difficult to perform (or avoided) and relate to their performance goals (“My hip ‘jams’ or ‘doesn’t feel right’ when I do a lunge to the left and this is impacting many poses in my Yoga practice”), or tasks which create respiratory or urogynecological symptoms (“I get short of breath in spin class, I leak urine when I jump,”).
- Any potential cognitive or emotional barriers to recovery (thoughts and feelings) or significant medical considerations.
Screening Tasks
Screening tasks are then chosen based on the meaningful task and these are charted on the outer circle of the Clinical Puzzle. For example, if the meaningful complaint is low back pain aggravated by sitting then three useful screening tasks that are components of this meaningful task would be:
- Standing posture (the position from which the task begins)
- Squat
- Sitting posture
Regional areas of the whole body are then assessed in each of the screening tasks to determine if the strategy is optimal or suboptimal. An optimal strategy for any task will:
- have optimal alignment, biomechanics and control throughout the entire body,
- distribute and balance pressure in all three canisters (cranium, thorax, abdomen),
- support optimal respiration, continence and pelvic organ support, and
- permit sufficient mobility to accommodate perturbations to the system (breath, movement, disturbances in the foundation of support
Optimal strategies look and feel good.
Optimal strategies for the transference of load through the low back and pelvis will support musculoskeletal, urogynecological and respiratory health. Suboptimal strategies produce sites that fail to transfer load and they often demonstrate poor alignment, biomechanics and/or control, or are associated with excessive increases in pressure (intra-abdominal, intra-thoracic, intra-cranial), poor breathing patterns (e.g. breath holding, limited chest wall expansion) or rigidity, mobility inappropriate for the intended task. Suboptimal strategies simply do not look good nor do they feel good.
Finding the Driver

When possible, the timing of loss of alignment, biomechanics and/or control (failed load transfer (FLT)) between the various sites of is assessed. (Fig. 3). Then specific manual and verbal cues/corrections are provided to one or more sites of failed load transfer to determine which correction has the most positive impact (e.g. improvement in range of motion, decrease in effort, reduction in symptoms) on the screening task. The pelvis is corrected/controlled by manually restoring neutral alignment in the transverse, sagittal and coronal planes, centering the pelvis over the base of support (feet) and then providing gentle compression. The patient then repeats the screening task to assess the impact of this correction on their ability to maintain optimal alignment of the thorax and move the hips.
The thorax is corrected/controlled by manually restoring neutral alignment in the transverse, sagittal and coronal planes with the corrections applied specifically to the thoracic ring (Lee D G 2015, Lee L-J 2003) and the screening task is repeated to assess any change in the performance of other sites of FLT. An enquiry is made as to the difference in the ‘gestalt of the experience’ when various body regions are corrected/controlled to not only confirm the hypothesis but to help the patient become aware of the differing experiences of their body when sites distant from their pain are corrected/controlled. Collectively, the timing and impact of various corrections on the screening determines the best place to focus further assessment for this individual, for this specific task. In the Integrated Systems Model approach this is called ‘finding the driver’ for that task. The patient is encouraged to focus on changes in the experience of the task (effort, ease, ability to breathe, pressure) rather than pain with respect to the appropriateness of a correction. It is possible to have low back pain be driven from the pelvis, thorax, foot, hip and even the cranium. While common patterns do exist, every low back pain patient is unique.
Once the driver is confirmed, the meaningful task is repeated to:
- confirm the hypothesis of the best place to begin treatment,
- create patient confidence and understanding as to how the regions of the body relate to each other and why sometimes treatment has to begin far distant from the site of their symptom(s), and to
- give the patient a different experience (gestalt) of their body and thus begin to change/reset their ‘brain map’ and re-conceptualize their body.
Changing motor output begins by changing the sensory input.
The next step is to determine the specific, or combination of, system impairment(s) (articular, neural, myofascial, visceral, cognitive/emotional) responsible for ‘driving the driver’ and the suboptimal strategy for their meaningful task.
The Integrated Systems Model and Muscle Recruitment Strategies (Motor Control)
Multiple studies suggest that the response to back pain is individual and task specific (Hodges 2011, Hodges, Van Dillen, McGill, Brumagne, Hides, Moseley 2013) although there are common features to most clinical presentations. Hodges notes that back pain patients present with a ‘redistribution of activity within and between muscles (rather than inhibition or excitation of muscles in a stereotypical manner)’ (Hodges 2011). All of the multisegmental muscles of the trunk contribute to movement and control and when their activity is redistributed they can produce specific vectors of force that contribute to thoracic ring shifts/rotations and pelvic rotations.
If the goal of rehabilitation (e.g. using motor learning strategies) is to modify the adaptation (remove, modify or enhance) then this needs to be considered on an individual basis with respect to the unique solution adopted by the patient (Hodges 2011 p 222-223).
The best way to illustrate how the Integrated Systems Model considers where, when, and how to modify the adaptation individually is through individual case reports. The videos of these case reports can be found in the online lecture accompanying this article.
Case report #1
Ms. A presented with right-sided lumbopelvic pain (meaningful complaint) aggravated by walking (meaningful task). The single leg standing task was chosen as an initial screening task to assess her strategies for vertical loading through her low back and pelvis. She had three sites of failed load transfer during right single leg standing: the right SIJ (the right innominate rotated anteriorly relative to the sacrum), the right hip (the femur translated anterior when she shifted her weight to the right) and the 6th thoracic ring (translated to the left/rotated to the right).
The 6th thoracic ring was found to be the driver because it failed first and when corrected resulted in improved position and control of both the right hip and the right SIJ. Neither a right hip nor a pelvic correction improved the alignment or control of the 6th thoracic ring during right one leg standing.
Over-activation of a specific fascicle of the right iliocostalis (from the right iliac crest to the right 6th rib) combined with under-activation of the right transversus abdominis (TrA) was the noted neural system impairment. When the 6th thoracic ring was manually corrected, the activation of the right TrA improved. Ms. A’s treatment included release techniques and exercises to restore the alignment, biomechanics and control of her 6th thoracic ring during tasks necessary for walking. No specific training was needed for the right TrA at this time since she was able to control the alignment, biomechanics and control of the right SIJ during single leg loading when the 6th thoracic ring position was corrected and controlled, and the recruitment strategy of this deep trunk muscle was improved when the 6th thoracic ring was aligned and controlled.
Case report #2
Ms. T is a 25-year-old nurse who did CrossFit Training five to six times per week and as a consequence of this high intensity training had experienced multiple muscle strains and injuries. As her ability and training increased she noticed increasing lumbopelvic pain, urinary urgency and frequency. Recently, she noticed that if she does not void often she experiences stress urinary incontinence especially with tasks that load the trunk or increase her intra-abdominal pressure (i.e. box jumps). Ms. T was nulliparous.
Meaningful Complaint
Primary concerns for Ms. T included the increasing frequency of her need to void and the increasing incidence of stress urinary incontinence during her CrossFit training. She voiced concern about the impact of future pregnancies on her urinary health and lumbopelvic pain.
Meaningful Task & Screening Tasks
Ms. T’s meaningful task was a box jump and the tasks chosen to evaluate for strategy were standing posture and a squat task since each of these directly relate to her meaningful task. Ms. T stood with her pelvis rotated in the transverse plane to the right (TPR right). Her lower thorax (thoracic rings 8 to 10) was rotated to the left (TPR left lower), the 7th thoracic ring was rotated to the right, and the 6th thoracic ring was rotated to the left.
Correcting the alignment of the 6th and 7th thoracic rings improved the position of the pelvis (reduced the right TPR), while correcting the alignment of the pelvis increased the left rotation of the lower and mid thorax. The 6th and 7th thoracic ring alignment did not improve with correction of the pelvis. This suggests that the thorax is driving the pelvic position as opposed to the pelvis driving the thorax and that further investigation of what is causing the mal-alignment of the 6th and 7th thoracic rings was needed.
During a squat, the following sites of failed load transfer (suboptimal alignment, biomechanics or control) were noted including the timing of when they failed:
- The 7th thoracic ring rotated to the right and the 6th thoracic ring rotated to the left before
- the left SIJ gave way (i.e. the left innominate anteriorly rotated relative to the sacrum).
When the alignment of the 6th and 7th thoracic rings was corrected, the left SIJ no longer failed. In comparison, when the left SIJ was controlled, the 6th and 7th thoracic rings continued to rotate during the squat task, a sign of failed load transfer. These findings suggest that the 6th and 7th thoracic rings were the primary driver for this task and that further assessment should focus on determining what was causing the loss of alignment, biomechanics and control of the 6th and 7th thoracic rings.
The supine bent leg raise task is not relative to her meaningful task of box jumping; however, for Ms. T to know if she is correcting her thoracic rings properly, it will be useful as part of her exercise training. Ms. T found that more effort was required to lift her left leg (with the knee bent) than her right. No change in effort was noted when the right TPR of her pelvis was corrected. However, the task was much easier to perform when the 7th thoracic ring was corrected. In the supine position the 6th thoracic ring position automatically corrected when the 7th thoracic ring alignment was improved manually.
Hypothesis of Ms. T’s Primary Driver
Correction of the 6th and 7th thoracic rings improved the performance of Ms.T’s standing posture, squat task and the ability to lift her left leg while supine; therefore, these thoracic rings were hypothesized to be the primary driver. Further system analysis (neural, articular, myofascial, visceral (or combination)) was required to determine what was causing the suboptimal alignment of the 6th and 7th thoracic rings across multiple tasks.
Vector Analysis of Ms. T’s Primary Driver
When correcting the 6th and 7th thoracic rings, a resistant vector of force was felt from the left side of her upper abdominal wall. On palpation, increased resting tone was noted in the left external oblique. The over-activation covered a number of thoracic rings and was regional, not fascicle specific. However, the primary impact was on the 7th thoracic ring. A specific fascicle of the external oblique has the ability to anteriorly rotate one rib. This rib, however, is part of an entire thoracic ring (Lee 1994) such that when the rib anteriorly rotates on the left, it can potentially produce left translation and right rotation of the entire thoracic ring (Fig. 4). When the 7th thoracic ring was corrected, the 6th thoracic ring self-corrected, suggesting that the primary impaired thoracic ring was the 7th.

The next question was, What was the impact of this over-activation of the left external oblique on the recruitment strategy of the entire abdominal wall?
Analysis of Ms. T’s Abdominal Wall
More palpable tension was noted superficially on the left side of Ms.T’s lower abdomen, likely due to the over-activation of the left external oblique (EO) muscle. When asked to gently contract her pelvic floor, further activation of the left EO was palpable as an immediate first response.
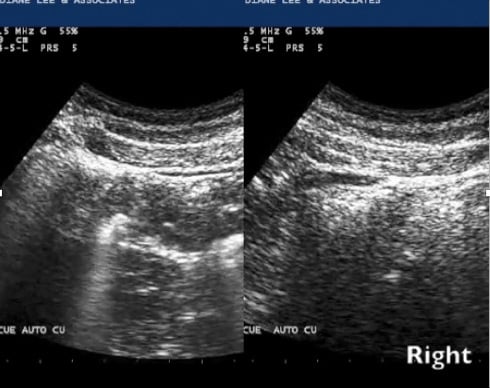
Ultrasound imaging revealed that the right TrA responded appropriately to this cue and the left TrA did not (Fig. 5).
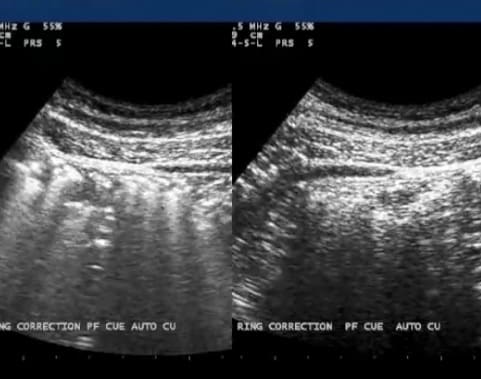
When the 7th thoracic ring was corrected manually, there was less superficial abdominal tension and an improved, more symmetric activation of both the left and right transversus abdominis was felt and seen via ultrasound imaging (Fig. 6). Although improved, the ‘robustness’ of the TrA activation was less on the left.
Analysis of Ms.T’s Pelvic Floor
A transabdominal sagittal view of the pelvic floor contraction did not reveal any asymmetry since only the midline of the bladder and pelvic floor are imaged with this orientation. A good lift in an optimal location for urethral and bladder support was noted. A perineal real-time ultrasound view of Ms. T’s pelvic floor contraction when her pelvis was rotated (right TPR) revealed less lift (decreased amplitude) and less pelvic organ support during her cough (greater descent seen) compared to when her pelvis was in a neutral position.
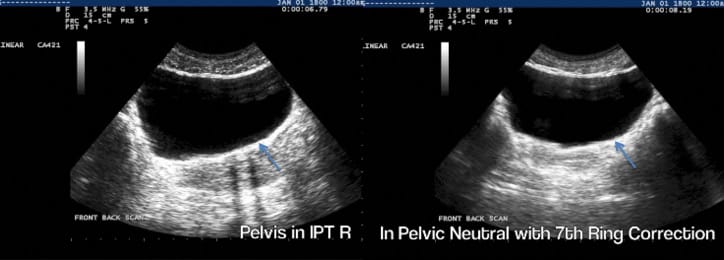
A transabdominal transverse plane view (Fig. 7) revealed that when Ms. T’s pelvis was rotated in the transverse plane, no lift of the left side of her levator ani was apparent when she was asked to contract her pelvic floor (left image of the figure – the right side of the image is the left side of the bladder/pelvic floor). This was confirmed with intra-vaginal palpation. When the 7th thoracic ring was manually corrected (thus reducing the right TPR of the pelvis) the shape of the bladder base was more symmetric, as was the pelvic floor lift; however, she could only hold this contraction on the left for 5 seconds (endurance deficit). Weakness and loss of endurance of the left side of the levator ani was still present in spite of removing the influence of the right transverse rotation (TPR) of the pelvis on the recruitment strategy.
Hypothesis of Tiana’s Story
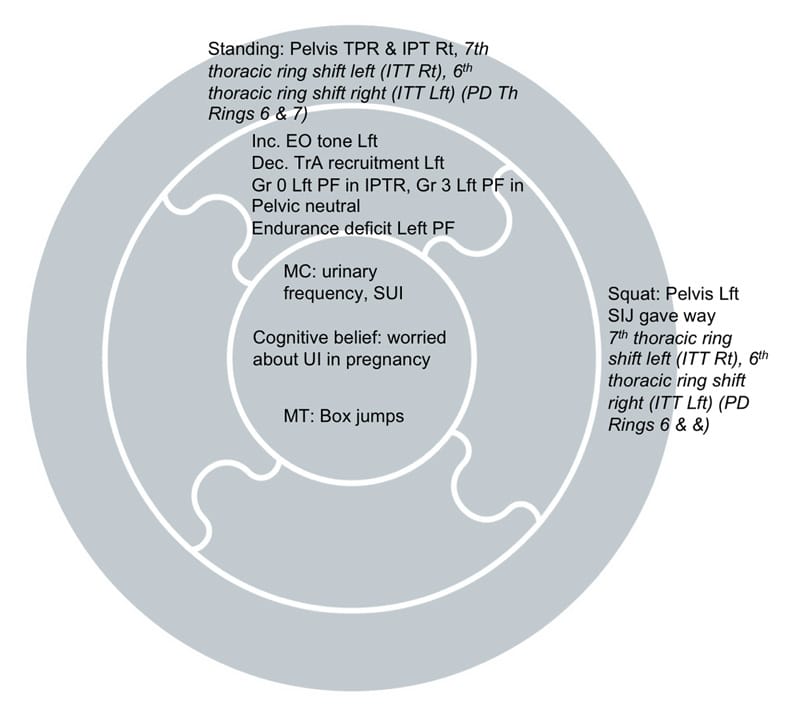
The hypothesis was that Ms. T had a redistribution of activation of the muscles of the abdominal wall and pelvic floor (over-activation of the left external oblique, under-activation of the left transversus abdominis, reduced activation and relaxation of the left iliococcygeus). Although the recruitment strategy of the deep muscles of the lumbopelvis improved when the right TPR of the pelvis was corrected, there was an underlying strength and endurance deficit on this side of both her abdominal wall and pelvic floor. Collectively, all of this was creating poor urethral, bladder, pelvic, 6th and 7th thoracic ring support during tasks which increased loading through the pelvis and its organs (i.e. the box jump). Her complete Clinical Puzzle is illustrated in figure 8.
Treatment
According to the treatment principles of the ISM approach, the first step was to release the vectors that were creating suboptimal alignment of the 7th thoracic ring and then restore better recruitment synergies for the abdominal wall and pelvic floor.
Release the left external oblique and align the 6th and 7th thoracic rings
Home exercise:
- Supine: hook lying – align the 7th thoracic ring and then breathe with a lateral costal expansion strategy for 3 to 4 breaths. Then, take the legs to the right on the inhale breath, hold, and on the exhale breath connect to TrA and the PFM and return the legs to neutral for 3 to 4 repetitions. Then, recheck the effort it takes to lift the left leg; it should be less.
- Side angle pose: position the left leg back and correct the 7th thoracic ring first. Next, unwind the right TPR, then rotate the thorax to the left to lengthen the left EO; hold this position for 3 breaths.
Connect/control and move
Home exercise:
- Correct the alignment of the 7th thoracic ring, co-activate the pelvic floor and TrA (feel for the co-contraction of the left side of the levator ani and abdominal wall (as well as the right)) and then perform three squats. The previous three exercises should be done before her CrossFit Training workout.
Strength and endurance training for the pelvic floor
Home exercise:
- Left side levator ani/TrA strength and endurance training: work up to 10 repetitions of 10 second holds in pelvic neutral, 3 times per day, at least 3-4 times per week. Introduce both slow and fast co-contractions specific for CrossFit Training after 4 to 6 weeks. Continue with intensive specific PF/TrA muscle training for at least 8 weeks
Follow-up Plan: Reassess symmetry of activation (motor control), strength and endurance (performance) of the levator ani/transversus abdominis in 4 to 6 weeks, along with the ability to control the left SIJ, 6th and 7th thoracic rings and maintain urethral closure during squats and box jumps. Progress training to more advanced thoraco-pelvic alignment and loading exercises as necessary at that time.
Summary
In closing her keynote presentation at the 2012 IFOMPT conference in Quebec, Professor Gwen Jull said:
The advantage of a clinical reasoning approach is that it is responsive to new knowledge and evidence, is flexible and allows for change and growth (Jull 2012).
The Integrated Systems Model is such a clinical reasoning approach. It is a framework, not a classification, that considers all three dimensions of the patient’s experience and the barriers that each may present to the recovery process for both acute and persistent conditions.
In closing her presentation at the 2016 World Congress on Low Back and Pelvic Pain in Singapore, Professor Julie Hides said the clinical reasoning process was critical for the management of individual patients and that:
The Integrated Systems Model, which draws from several other approaches, may provide a very useful framework for clinicians which could incorporate individual aspects of the evidence based approaches presented.
 The Integrated Systems Model, which draws from several other approaches, may provide a very useful framework for clinicians which could incorporate individual aspects of the evidence based approaches presented.
The Integrated Systems Model, which draws from several other approaches, may provide a very useful framework for clinicians which could incorporate individual aspects of the evidence based approaches presented.
The body/person can no longer be considered as individual ‘parts or problems’ in either assessment or treatment. Most tasks involve the whole body, thus assessment must include analysis of the relationship between the body regions and the impact and inter-play of each. Finding drivers requires the skill to not only interpret a finding but to find it reliably.
For clinicians, visual and kinesthetic perceptions are foundational tools for assessing the human form in function. Understanding our individual strengths, weaknesses, accuracies and misperceptions enhances our reliability and skills necessary to find a finding. Clinical reasoning of the findings then determines its relevance to the clinical picture, which subsequently directs management of individual patients. While clinical reasoning can be taught through texts and online media, there will always be a need for hands-on practical courses; this is the art and skill of physiotherapy that is so difficult to measure with science.
To become really skilled in the ISM approach, come learn with me on the ISM Series offered annually in Akasha and in one other location world-wide each year.
Diane Lee
Learn with Diane Lee
Diane Lee and Associates, Surrey, B.C. Canada
References
Hodges P W 2011 Pain and motor control: From the laboratory to rehabilitation. Journal of Electromyography and Kinesiology: Official Journal of the International Society of Electrophysiological Kinesiology,.21(2):220–228
Hodges P W, Van Dillen L, McGill S, Brumagne S, Hides J, Moseley L 2013 Integrated clinical approach to motor control interventions in low back and pelvic pain. Ch. 21 in: Hodges P W, Cholewicki, J, Van Dieen J H (eds) Spine control: the rehabilitation of back pain, state of the art and science. Edinburgh, Elsevier p 265
Hodges P W, McGill S, Hides J A 2013 Motor control of the spine and changes in Pain: debate about the extrapolation from research observations of motor control strategies to effective treatments for back pain. Ch. 20 in: Hodges P W, Cholewicki, J, Van Dieen J H (eds) Spine control: the rehabilitation of back pain, state of the art and science. Edinburgh, Elsevier p 234
Jones M A, Rivett D 2004 Introduction to clinical reasoning. In: Jones M A, Rivett D A (eds) Clinical reasoning for manual therapists. Edinburgh, Elsevier p 3
Jull G 2012 Management of cervical spine disorders: where to now? IFOMPT Quebec City, Canada
Lee D 1994 Manual Therapy for the Thorax. www.dianelee.ca publishers, Surrey
Lee D 2011 The Pelvic Girdle, An Integration of Clinical Expertise and Research, Edinburgh, Elsevier
Lee D 2015 Highlights from an integrated approach to the treatment of pelvic pain and dysfunction. Ch. 17 in: Magee D J, Zachazewski J E, Quillen W S, Manske R C (eds) Pathology and intervention in musculoskeletal rehabilitation, 2nd edition. Edinburgh, Elsevier (at press)
Lee D G 2015 Biomechanics of the thorax – research evidence and clinical expertise. The Journal of Manual & Manipulative Therapy. 23(3):128–138
Lee D G, Lee L J, McLaughlin L M 2008 Stability, continence and breathing: The role of fascia following pregnancy and delivery. Journal of Bodywork and Movement Therapies 12:333
Lee D, Lee L-J 2011 Techniques and tools for assessing the lumbopelvic-hip complex. Ch. 8 in: Lee D The Pelvic Girdle, 4th edn, Edinburgh, Elsevier
Lee L-J 2003 Restoring force closure/motor control of the thorax, Ch. 7 in: Lee D The Thorax – An Integrated Approach, Diane G. Lee Physiotherapist Corp, White Rock
Lee L-J, Lee D 2011 Clinical Practice – The Reality for Clinicians. Ch. 7 in: Lee D 2011 The Pelvic Girdle, 4th edn. Edinburgh, Elsevier
Melzack R 2001 Pain and the neuromatrix in the brain, Journal of Dental Education, 65(12):1378
Melzack R 2005 Evolution of the neuromatrix theory of pain. The Prithvi Raj Lecture: Presented at the third World Congress of World Institute of Pain, Barcelona 2004. Pain practice: the official journal of World Institute of Pain, 5(2):85
Moseley L 2013 Trunk muscle control and back pain: chicken, egg, neither or both? Ch. 11 in: Hodges P W, Cholewicki, J, Van Dieen J H (eds) Spine control: the rehabilitation of back pain, state of the art and science. Edinburgh, Elsevier
Sackett D L, Straus S, Richardson W S, Rosenberg, Haynes R B 2000 Evidence-based medicine. How to practice & teach EBM. New York, Elsevier
Siegel D 2010 Mindsight. Bantam Books. New York
Van Dillen L, van Tulder M 2013 Targeting interventions to patients: development and evaluation. Ch. 17 in: Hodges P W, Cholewicki, J, Van Dieen J H (eds) Spine control: the rehabilitation of back pain, state of the art and science. Edinburgh, Elsevier p 195